
SDOH Glossary
Explicit Bias: The person is very clear about his or her feelings and attitudes, and related behaviors are conducted with intent. This type of bias is processed neurologically at a conscious level as declarative, semantic memory, and in words. Conscious bias in its extreme is characterized by overt negative behavior that can be expressed through physical and verbal harassment or through more subtle means such as exclusion. An example of explicit bias is someone placing a “No Gays Allowed” sign on their storefront and refusing services for members of the LGBTQ&+ community.
Implicit Bias:– Implicit or unconscious bias operates outside of the person’s awareness and can be in direct contradiction to a person’s espoused beliefs and values. What is so dangerous about implicit bias is that it automatically seeps into a person’s affect or behavior and is outside of the full awareness of that person. Implicit bias can interfere with clinical assessment, decision-making, and provider-patient relationships such that the health goals that the provider and patient are seeking are compromised. An example of implicit bias is that often overweight people are labeled as lazy, weak, and lacking self-control. Healthcare professionals may blame serious health issues on weight, therefore, unintentionally ignoring other possible causes.
National Center for Cultural Competence: Two Types of BIas
Cultural Competency: The integration and transformation of knowledge about individuals and groups of people into specific standards, policies, practices and attitudes used in appropriate cultural settings to increase the quality of services with the intention of producing better outcomes.
Cultural competence - Definition and Explanation - The Oxford Review - OR Briefings
Cultural Humility: A process of self-reflection and self-critique whereby the individual analyzes their beliefs and systems and works to understand those of others so that they can provide services that are trauma-informed, respectful, as well as both culturally and linguistically appropriate. Our SDOH program has training modules we can offer to support education for healthcare and community partners.
Diversity: Describes the myriad ways in which people differ, including the psychological, physical and social differences that occur among all individuals, such as race, ethnicity, nationality, socioeconomic status, education, age, gender, gender identity or expression, sexual orientation, marital status, mental and physical ability and learning styles. A diverse workforce creates an inclusive environment where perspectives are valued and individuals have the right to access culturally relevant information, resources and services that result in optimal health outcomes.
Environmental Justice: The fair treatment and meaningful involvement of all people regardless of race, color, national origin, or income, with respect to the development, implementation, and enforcement of environmental laws, regulations and policies. This goal will be achieved when everyone enjoys the same degree of protection from environmental and health hazards, and there is equal access to the decision-making process to have a healthy environment in which to live, learn, and work.
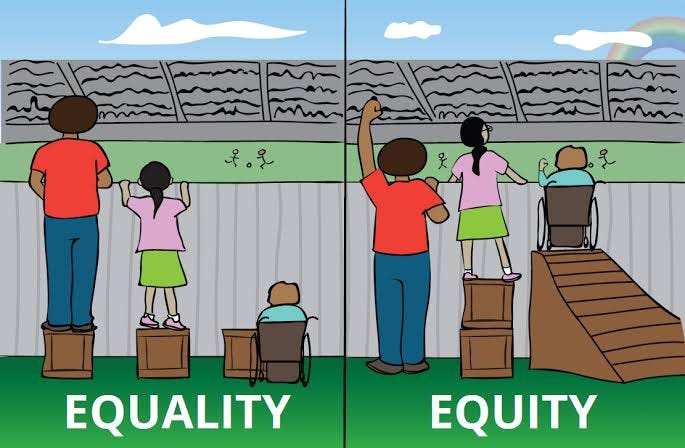
Equality: The condition under which every individual is treated in the same way, and is granted the same rights and responsibilities, regardless of their individual differences. It means giving everyone the same tools or opportunities.
Equity: When everyone, regardless of who they are or where they come from, has the opportunity to thrive. This requires eliminating barriers like poverty and repairing injustices in systems such as education, health, criminal justice and transportation. https://cdphe.colorado.gov/ohe
Equity vs. Equality: Equity represents impartiality, the distribution is made in such a way to even opportunities for all the people. Conversely, equality indicates uniformity, where everything is evenly distributed among people.
Food Security: “Food security (is) a situation that exists when all people, at all times, have physical, social and economic access to sufficient, safe and nutritious food that meets their dietary needs and food preferences for an active and healthy life.” (Food and Agriculture Organization of the United Nations. Trade Reforms and Food Security: Conceptualizing the Linkages. Food and Agriculture Organization of the United Nations; Rome, Italy: 2003. p. 313.)
Food Sovereignty: The right of peoples to healthy and culturally appropriate food produced through ecologically sound and sustainable methods, and their right to define their own food and agriculture systems. It puts the aspirations and needs of those who produce, distribute and consume food at the heart of food systems and policies rather than the demands of markets and corporations.
Health disparities: A health disparity is a specific kind of health difference that is strongly connected to social, economic, or environmental disadvantages. These disparities negatively impact groups of people who have consistently faced greater barriers to good health due to factors such as race or ethnicity, religion, income level, gender, age, mental health, disabilities (cognitive, sensory, or physical), sexual orientation or gender identity, geographic location, or other characteristics that have historically been tied to discrimination or exclusion. (co-pilot, 2026; rephrase Healthy People 2030).
Inclusivity: The practice or policy of providing equal access to opportunities and resources for people who might otherwise be excluded or marginalized, such as those having physical or intellectual disabilities or belonging to other minority groups. An inclusive environment and inclusive care is when diversity is leveraged to create a fair, healthy and high-performing organization or community. It also enables individuals and groups to feel safe, respected, engaged, motivated, and valued for who they are and for their contributions toward organizational and societal goals.
Disability Inclusivity: Disability inclusion refers to the meaningful participation and integration of individuals with disabilities into all aspects of society, ensuring they have equal access to opportunities, resources, and services.
The Need for Public Health and Inclusivity in Divisive Times
Intergenerational Trauma: The concept developed to help explain years of generational challenges within families. The transmission (or sending down to younger generations) of the oppressive or traumatic effects of a historical event. As generational cycles occur, negative patterns and traits are known to transfer through multiple generations via learned behavior, family dynamics and environment. Historical examples of groups affected by generational trauma include Black Americans, Holocaust survivors, and Indigenous communities, among others. In Montana, we are especially aware of the intergenerational and unconscious grief experienced by Indigenous peoples passed from generation to generation due to forced relocation, land dispossession, and loss of spiritual practices, language and culture.
Racism: Any distinction, exclusion, restriction or preference based on race, colour, descent, or national or ethnic origin that has the purpose or effect of nullifying or impairing the recognition, enjoyment or exercise, on an equal footing, of human rights and fundamental freedoms in the political, economic, social, cultural or any other field of public life.
Institutional: Institutional racism describes the ways in which a society’s systems and organizations—often without intending to—consistently advantage certain groups while disadvantaging others in terms of access to opportunities and important resources. It highlights how discrimination can be embedded in everyday structures and practices, even when no individual is deliberately trying to exclude anyone. Institutional racism harms health by shaping access to care, quality of treatment, living conditions, and exposure to chronic stress. These effects are measurable across many health outcomes, including maternal mortality, chronic disease, and life expectancy. https://www.ebsco.com/research-starters/sociology/institutional-racism
Structural: Structural racism arises from a system in which public policies, institutional practices, cultural norms, and everyday assumptions interact to maintain racial inequality. It has long been embedded in the social, economic, and political structures that shape our lives. Structural racism affects health because it shapes the conditions in which people are born, grow, live, work, and age. It influences exposure to risks, access to care, and the resources needed for good health. The result is predictable, measurable, and persistent racial health inequities.
Structural Barriers:
Structural barriers are obstacles that unfairly impact certain groups more than others and keep major gaps in outcomes in place. These barriers include policies, practices, and social norms that give advantages to one group while consistently disadvantaging another.
Upstream/Downstream Interventions: We often discuss health using the metaphor of a stream, with upstream factors bringing downstream effects. Social needs interventions create a middle stream. It is not a choice, of one over the other. We need social and economic interventions at both the community and individual level.
Upstream efforts aim to improve.
Midstream efforts seek to create individual-level impact by meeting individuals’ social needs through screenings, referrals, and other individually-focused processes/protocols. They are further upstream than medical interventions, but not yet far enough. Social workers, community health workers, and/or community-based organizations provide direct support/assistance to meet patients’ social needs.
Downstream efforts seek to create patient-level impact by providing clinical care. Redefining the meaning of “social determinants” to be mostly or only about the immediate social needs of expensive patients makes it harder to focus on the systemic changes necessary to address root causes of poor health.
Improvements in our nation’s health can be achieved only when we have the commitment to move even further upstream to change the community conditions that make people sick. The demand for social needs interventions won’t stop until the true root causes are addressed.


