
Partnerships for Success (PFS)
PFS Project Description
The Montana Department of Public Health and Human Services Behavioral Health and Developmental Disabilities Division (BHDD) strives to reduce youth substance misuse through SAMHSA’s Partnership for Success (PFS) Grant. The PFS grant uses the Strategic Prevention Framework to guide its work in high-risk communities throughout Montana.
Population & Focus Area
Montana PFS focuses on preventing youth ages from 9 to 20 years old from underage use of alcohol, marijuana, and methamphetamine.
Program Goals & Objectives
Goal 1: Prevent the onset and reduce the progression of substance abuse in youth ages 9-20 in funded counties, and for disproportionate populations (On Probation, In Foster Care and On Reservation).
Goal 2: Strengthen prevention capacity/infrastructure at the state, tribal and county levels.
Goals 3: Strengthen comprehensive prevention approach.
Introduction to the Strategic Prevention Framework
The Strategic Prevention Framework is SAMHSA’s five-step planning process for instituting an intervention in your community, region or state. There are five steps, and each is guided by principles of sustainability and cultural competency. Sustainability meaning the process of an effective system achieving and maintaining desired long-term results. Cultural competency refers to a defined set of values and principles that encourage behaviors, attitudes, policies and structures that enable an organization to work effective cross- culturally.
Prevention Specialist Training: Substance Abuse Prevention Skills Training (SAPST)
SAPST training introduces the fundamentals of substance abuse prevention based on the current knowledge and practice in the field. The training was developed for individuals new to substance abuse prevention or early in their prevention career. In addition to the four days of training, participants will also be sent a link and need to complete an on-line course prior to the training.
For a brief introduction to the principles of the SPF process: please visit the SAMHSA website.

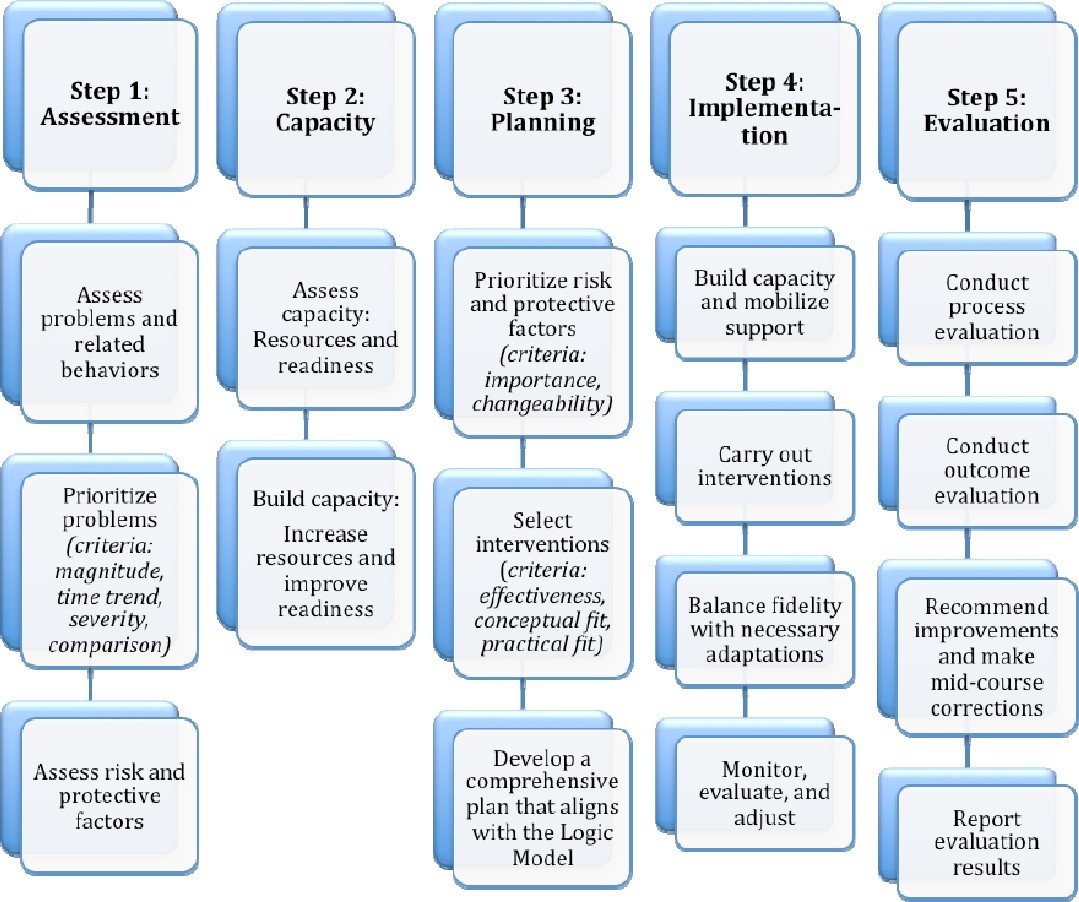
The five steps of the SPF include:
- Assessment: Collect data to define behavioral health problems and needs within a geographic area.
- Capacity: Mobilize and/or build capacity within a geographic area to address identified needs.
- Planning: Develop a comprehensive, data-driven plan to address problems and needs identified in assessment phase.
- Implementation: Implement evidence-based prevention programs, policies, and practices.
- Evaluation: Measure the impact of implemented programs, policies and practices.
Sustainability and cultural competence should be integrated into all steps of the SPF.
